by Andrew I Spielman
How to cite this page: Spielman, AI. History of Oral Surgery. In: Illustrated Encyclopedia of the History of Dentistry. 2023. https://historyofdentistryandmedicine.com/
Today, an oral surgeon employs sophisticated techniques that involve extractions, dentoalveolar surgeries, soft and hard tissue pathologies, and orthognathic corrective surgeries, to name a few. The history of oral surgery has to be separated into extractions and everything else a surgeon does today. Tooth extraction was primarily the domain of tooth drawers and barbers from the 11th century. Surgery involving more complicated conditions, including traumas, was the work of more specialized individuals, like barber surgeons or surgeons. Head and neck surgery, due mainly to trauma, predates extractions. While evidence of extraction dates to the first century Rome, trauma surgery goes back to the middle of the 2nd millennium BCE.
The Edwin Smith Papyrus, one of the oldest compilations of surgical interventions, dates to ~1500 BCE, describing 48 trauma cases, listing 27 that deal with head, nose mandible, ear, and lip trauma and six more cases report on the trauma of the throat and neck (1). All told, 33 of the 48 trauma cases, almost 70% are the domain of head and neck surgery. The Edwin Smith Papyrus is the first “textbook” of head and neck surgery.
Tooth extraction in Ancient China was practiced according to the early first millennium BCE classic Nei Ching of the Yellow Emperor’s Textbook of Medicine (2).
In antiquity, surgery was looked upon as a separate branch of medicine. Even at the time of Hippocrates, removing a stone was considered tabu for physicians to be engaged in, as it was made clear in the Hippocratic Oath (“I will not cut for stone, even for the patients in whom the disease is manifest; I will leave this operation to be performed by practitioners”).
The formal separation between physicians and surgeons occurred with the 1092 Papal decree when Cyril II of Alexandria invited barbers to ensure the hair grooming needs of priests and monks. During the next 120 years, two additional Popes (Alexander III in 1163 and Innocent III in 1215) enforced the rule of barbers overseeing haircutting and other procedures that might involve bleeding. In effect, the decrees prohibited priests from being involved in surgical interventions that lead to bleeding (ecclesia abhorrent a sanguine – the Church is horrified of blood) (3). The separation of physicians and surgeons ended in 1794; the post-revolution, newly organized school of medicine in Paris, Ecole de Santé, reunited medicine and surgery (4).
The separation of the tooth drawers from barbers is far less clear. Barbers continued to extract teeth, even when more specialized functions were added, such as amputations, bloodletting, leeching, or cupping. Both tooth drawers and barber-surgeons practiced extractions, the latter becoming more organized and regulated over the centuries.
The first tooth extractions appeared recorded in the 4th century BCE, during the time of Hippocrates, to remedy dental pain when other, less invasive steps could not help. Forceps and tweezers were called rizagra by the Greeks and vulsella by the Romans (5). The name vulsella comes from the name of the Finger Oyster, a bivalve in Latin Vulsella vulsella.
History of the Forceps, Elevator, Toothkey and Pelican
Although forceps were available (6), the preferred extraction mode was with two fingers. When forceps were used to avoid the fracture, the cavitated teeth first, were filled with wood fiber and lint or lead (5). Cornelius Celsus (25 BCE-50 CE), a Roman physician, describes methods to loosen up carious teeth so they can easily be removed with fingers. He recommends two recipes: peppercorn or ivy berry placed inside the cavity and a pulverized, resin-mixed tailbone of a stingray (trigon or pastinaca) (7). Using fingers for extractions also fits with finding a cache of extracted and deeply carious teeth in the sewer under a shop in the Roman Forum. The 86 teeth, almost all intact, likely came from at least 50 individuals. Their appearance indicates a highly skilled tooth drawer on the Forum and a gentle technique (8).
Nevertheless, forceps were used, as evidenced by findings in Greek and Roman graves. They have been forged by blacksmiths and, based on their simple design, used as a universal tool for all teeth. Forceps were also used in the 3rd-century School of Alexandria. The technique survived well into early Medieval times. Galen, Celsus, the Islamic physicians, and later, de Chauliac and Pará all described using forceps for extractions.

Figure – Extracted teeth found in a drain pipe of a shop on the Roman Forum (based on Becker, 2014). A 1st c. Roman forceps (upper left corner). These teeth were most likely loosened by hand first.
Finger extractions were not unique to Rome or Greece. It was also employed in Ancient China and Japan (9) and is still used 1000 years later. Abulcasis (936-1013), the preeminent Arab physician and surgeon of Cordoba, in the last volume of his 30-volume Kitab al-Tsarif, describes the method and positioning of the patient for extraction. In a section entitled: De extractione doloris dentium, he advises: sedere infirmum inter manus tuas et caput eius in sinu tuo et rade molam et dentem. (Translated: position the patient’s (head) between your hands, (place) the patient’s head in your lap, and loosen up the gum around the tooth) (10).
Abulcasis, for the first time, provides a rudimentary rendition of the forceps, elevators (top two images below), and a set of other instruments for extraction (11,12). In addition, Arab physicians of the 9th and 10th centuries, including Abulcasis, Ibn Sina, and Rhazes, described and illustrated the surgical removal of a ranula, stabilization of mandibular fracture, and cauterization of teeth.

Top two images – forceps and lancet- Abulcasis (11.12). Middle image – pelican, an extraction tool first appears in Guy de Chauliac’s Chirurgia Magna (13). Pelican – Pare, 1628, p.613.
Following the golden age of Arab medicine, descriptions of surgical techniques and the forceps reappear 250 years later in the work of Guy de Chauliac (1298-1368), the 14th-century surgeon at the University of Montpelier in the service of the Pope at Avignon. Although he adds little new to Abulcasis, in 1363, Chauliac is the first to describe the pelican as a hoop cramp in Chirurgia Magna (13), see the third image from the top above). Chauliac’s text includes only a short section on dental surgery, and no pelican illustration was available until the 1585 edition (14). Interestingly, the illustrations he displayed are adopted from the work of Ambroise Paré, published just ten years prior (15) (see image on the left taken from Pare, 1628, p.613).
Ambroise Paré (1510? -1590), one of the greatest surgeons of the Renaissance, was a practicing barber-surgeon in the service of four French kings. He designed new surgical instruments, extraction tools, obturators for cleft palate, gentle wound healing, and arterial ligation techniques. His life work entitled Oeuvres (Works) was published in 1575. His surgical sections are far more elaborate than the section on tooth replacement, which is limited to a few paragraphs. To treat partial edentulism, he recommends placing a small carved block of teeth made of ivory, hippopotamus, walrus bone, or narwhal tusk attached to neighboring abutment teeth using a gold wire or thread. Paré believed in the “tooth worm” (Et pour faire mourire les vers, faut appliquer choses caustique, ausi pyrethre destrampe en vinaigre, ou theriaque dissout en mesme liqueur: seront aussi appliquez ails, ou oignons, ou un d’aloe – And to kill the worms apply something caustic, hot, dissolved in vinegar or theriac dissolved in the same, or apply garlic, onion or aloe) (16). He was more comfortable as a surgeon. Restorative or prosthetic dentistry was less of a focus.
Peré’s main contribution was not just the synthesis of information and compilation of surgical methods and tools but also changes in wound dressing and ligation techniques. Paré was dubbed the gentle surgeon for changing the hot oil cauterization technique used by his predecessors to a more gentle wound dressing with a mixture of egg yolk, oil of roses, and turpentine (”un digestif fait de jaune d’oeuf, huile rosat, et terebenthine”)(16). This treatment was based on an accident when he ran out of hot oil during one of the battles. Similarly, Paré forgone hot iron cauterization of arterial bleeding. Instead, he re-introduced the ligature (17).
Guy de Chauliac and Ambroise Paré’s influence was felt over centuries. For instance, the illustration of the pelican, forceps, and elevators in the work of several surgeons of the 15th-16th century (Giovanni D’Arcoli (1412-1484), Walther Ryff (1500-1562), or Jacques Guilleameau (1550-1613)), were copied from Chauliac and Paré.
With all the advances in surgical instruments, extractions still needed to be widely used. They were considered a step of last resort and often ended up in the care of poorly educated tooth drawers. Patients also tried to avoid extraction because of a lack of anesthetic and the potential for collateral damage, infection, or bleeding. Queen Elizabeth I (1533-1603), who had famously ruined her teeth as a result of excessive sugar consumption, underwent extractions only after Aylmer, the Bishop of London, allowed a tooth drawer to extract one of his teeth to ensure the Queen that the pain was bearable (18).
Just as Paré made significant technical and conceptual advances in the 16th century, Johannes Scultetus (1595-1645), a German surgeon from Ulm, made advances in the 17th century. In 1655, his son published posthumously Armamentarium chirurgicum (Surgical tools) Scultetus’ work. Scultetus improved instruments and provided detailed descriptions of novel surgical techniques, including many for head and neck surgery.
Several 18th-century surgeons made a mark on the further development of instruments. Rene Jacques Croissant de Garangeot (1688-1759), a French surgeon, in 1727 published an important work on surgical instruments: Nouveau traité des instrumens de chirurgie les plus utiles et de plusieurs nouvelles machines propres pour les maladies des os (New study on the most useful surgical instruments and several new proper tools for bone diseases). The second volume of the work includes a series of dental elevators named after him, Le clef de Garengeot. The instruments include, for the first time, the probe to detect cavities (sonde) and lancets to remove decayed structures. Barely thirty years later, in 1754, Henry de Lécluse published Nouveaux elemens d’odontologie (New Elements of Dentistry), describing a surgical elevator that bears his name.
As surgical techniques of the head, neck, and oral cavity improved, medical books appearing in the 18th century on general surgery included sections on oral surgery. One important text was the 1739 edition of Lorenz Heister’s Institutiones chirurgicae – General System of Surgery (19). A significant moment in the history of oral surgery is the publication in 1778 of Anselm-Brechillet Jourdain’s (1734-1816) Traites des maladies et des operationes reellement chirurgicale de la bouche (Study on diseases and significant surgical operations of the mouth) the first text dedicated solely to dentoalveolar surgery. Similarly crucial for the 19th century was James Edward Garretson’s 1869 A System of Oral Surgery for Orthognathic Surgery, a text that dominated oral surgical education in the second half of the 19th century. That same year, Garretson established oral surgery as a specialty, the first within dentistry (20).
With all the advances in surgical instruments, during the 2500-year history of tooth removal, extractions employed only four tools: the forceps, the elevator, the tooth key, and the pelican. The forceps, the oldest instrument, is still in use today after two and a half millennia. The elevator is still in use for the last 1000 years since Abulcasis. The pelican was used for about 500 years, from Guy de Chauliac (1363) to the early 19th century, while the tooth key was employed only for about 100 years, from the mid-18th to mid-19th century. It was discontinued because of the potential damage, tooth fracture, and even jaw fracture it could cause. Additional instruments, screws, and multipurpose tools were introduced during the last 300 years. However, their use was short-lived and added relatively little to the overall advancement of the specialty.
For each of the instruments mentioned above, one can find several technical advances, improvements, and instruments that bore the name of their inventor or country. The reader is invited to consult excellent reviews on this subject (21). While the original design of the above-described instruments followed the principle of practicality and ease of use and transportation, safety and specificity became the focus in the design of instruments from the mid-19th century. A considerable change came in 1825 when Cyrus Fay’s designs improved extraction forceps (22). A more lasting change occurred in 1841 when John Tomes, the “Father of modern dental surgery in Britain” (1815-1895), significantly improved the anatomically accurate and specialized tools of extractions (23). For the last 150 years, the design of forceps and elevators has stayed relatively stable.
Extraction is just one aspect of dentoalveolar surgery. Sutures are another. The history of oral surgery sutures is identical to those in general surgery. The earliest devices for suturing were 60,000-year-old bone needles (see image to the left, below) for stitching together animal hides (24).

Figure 1A. Bone needles were used 60,000 years ago. 1B. Roman needle. Materials used for threads could be animal hair, tendons, or plant fibers. (Images in Wikimedia Commons, Muséé de Toulouse (1A), Wellcome Collection (1B).
The Edwin Smith Papyrus, from cc. 1600 B.C., a 15 feet long surgical text described 48 trauma cases, including five to the head, neck, and face requiring wound closure (#10, 14, 23, 26, and 28). The exact text translated in 1930 states, “Thou should draw together for him the gash with stitching“. The Edwin Smith Papyrus uses the symbol “ydr, ” interpreted as stitching together. (25) (Figure to the right). In Ancient Egypt, sutures were found in the bodies that underwent mummification or treatment following trauma. In either case, Egyptians used plant fibers, hair, tendons, or wool threads for sutures.

In the first millennium BCE (about 600 BCE), the ancient Indian text Susrata Samhita describes using giant ant (Eciton bruchelli) claws/pincers to hold the edges of a wound together (26). The giant ant is 3-12 mm long, and its mandibles are about 1-2 mm each. Once the live ant bit into the two sides of the wound, the head of the ant was cut off, holding the edges together (27). Susrata Samhita also describes bow strings made of sheep intestines in wound closure (26). Sheep intestines were used for string instruments. One such 3-stringed instrument derived from the Welsh word for “fiddle” was called “kitgut or kit string,” from which the word catgut was apparently derived.
In Ancient Greece and Rome, first mentioned by Galen, fibulae, similar to our safety pins, were inserted at two edges of the wound, and vegetable fibers or animal gut was passed around the protruding edges of the fibula in the form of eight, holding the wound together. Galen, a physician to several emperors and many gladiators, used catgut-type bow strings to suture the tendons of wounded fighters. Such techniques were also used by Arab physicians of the early medieval times for ruptured tissue or to stop bleeding; hot iron cauterization was equally employed for hemostasis. Ambroise Paré, the French barber-surgeon, “rediscovered” ligature using silk (28) instead of the more painful hot oil cauterization. In addition, his wound dressing technique was gentle. It included egg yolk, oil of roses, and oil of turpentine. It promoted better wound healing.
Along with animal gut, gold wires were also used for medieval sutures. As facial and oral surgery evolved out of general surgery, suturing techniques used in general surgery also made their way into dentoalveolar surgery.
With the introduction of aseptic surgery in 1867, Lister treated his suture material with chemicals. He recommended carbolic catgut. In 1906, iodine proved a better sterilizing agent for sutures. However, mass production started in 1887 when Johnson and Johnson introduced sterile sutures, gauze, and wound dressing.
In the 19th century, American physician Philip Syng Physick highlighted the importance of suture material absorption and popularized chromic sutures. Meanwhile, silver wire was introduced by James Marion Sims for closing tissue under tension. Silver sutures were easier to sterilize but more difficult to tie. By the 1930s, synthetic, non-absorbable suture materials became available. The first synthetic suture was made of polyvinyl alcohol, followed by polyester and polyglycolic acid sutures in the 1950s and 1960s. Starting in the 1960s, the Ethicon company introduced sterilization by irradiation (29).
In 1974, the non-absorbable sutures were replaced with synthetic absorbable sutures. They had complex braiding patterns to increase their strength. Additional advances in sutures took into consideration the specific specialty requirements. Vascular, abdominal, skin, or eye surgery all commercialized specific improvements in absorbability, strength, and post-surgical scar visibility.
In 1998, skin adhesives made their debut. They used cyanoacrylate to bond together the edges of a wound without the need for sutures. Adhesive bonds were fast, efficient, and reduced post-surgical wound infections. The latest evolution in wound closure does not even use sutures; they are wound closure devices that hold the tissue in place at multiple points using a barbed synthetic loop.
Almost as frequently as extractions, dental implant placement is one of the essential staples in the routine procedures of an oral surgeon. The history of implants involves several aspects: the procedure itself, the evolution of the materials used for implants, and the location and types of implants, including tooth reimplantations and transplantations.
Tooth transplantation and reimplantation were used from the 16th century to the early 19th century with varying degrees of success. Ambroise Paré, Pierre Fauchard, Louis Fleury Lecluse, and John Hunter, to name a few, all promoted it. The period literature described some successful cases, especially if teeth were reinserted early if there was a sufficient blood supply, and if surgical trauma, tissue damage, local infections, and post-surgical mobility were kept to a minimum. One can only speculate that without today’s scientific rigor, only successful cases made it primarily into published texts. Therefore, the success rate of transplantations and reimplantations at the time is hard to gauge. However, with the emergence in the 20th century of more successful alternatives, they were abandoned for more predictable and scientifically backed implants.
For the scope of this section, the history will be restricted only to artificial tooth implants. The first endosseous implant (alloplast) was discovered in 1931 by Dr. Frederick Wilson and Dorothy Popenoe, involved in the Mayan excavations at Playa de los Muertos in Honduras. The couple found a mandible with three sea shells alloplasts shaped like a wedge placed into the sockets of three incisors of a young woman. The mandible was dated to the 8th century CE. Bone deposits around the implants identified later by the Italian Amadeo Bobbio indicated that the alloplasts were done while the subject was still alive (30). The type of shell used for these alloplasts may have belonged to Tridacna, the largest living bivalve saltwater clam, whose shell was later successfully tested for osseointegration (31).
There are many names involved in the history of end-osseous implants. An early inventor was the Italian M. Maggiolo, working in Paris at the turn of the 19th century. In his 1807 book, written with an introduction M. Jourdan, professor at the University in Montpellier, Maggiolo, demonstrated the components of an artificial root (“racine artificielle”) for placement into the socket of the freshly extracted tooth. The artificial root was cast in gold and had the hallmarks of a potentially successful end-osseous implant (32).
During the 19th century, several authors, including Chapin Harris and Horace Hayden, attempted endosseous implants made of lead, porcelain, iridium, or gold, all with limited success.

In 1913 EJ Greenfield of Wichita, Kansas, made an important advance by creating an “artificial root that is permanent”. He drilled a cylinder-shaped space in the bone using a hole saw to make room for a precisely fitting gold cylinder basket with side holes (33). The design intended the growth of bone cells into the cylinder. At the top, the cylinder could accommodate a crown.
During the first decades of the 20th century, several new designs were attempted using various materials. However, the lack of understanding of biocompatibility and tissue reaction to a foreign object led to limited success. A noteworthy improvement came in 1933 from the brothers Alvin and Moses Strock of Boston with careful experiments in dogs and humans testing with Vitallium, chrome-cobalt implant screws. Another significant improvement of the endosteal implant came in 1940 from the Italian Manlio Formiggini, whose spiral stainless steel wire design was meant to spur bone growth into the open space. The lack of predictable success with endosteal implants led to attempts with subperiosteal implants. In 1938 the Swedish Gustav Dahl attempted the first such implant. His pioneering steps were further improved by implant designs and better techniques, including that of Lenard Linkow of New York University, who began placing blade-designed implants in the early 1960s (34).
The materials used for successful implants were relatively few. A notable improvement was titanium. Discovered as titanium dioxide in 1791 by reverend William Gregor, it was named after the Greek mythological figures, the Titans, in 1795 by Martin Heinrich Klaproth, a German chemist. Pure titanium metal was obtained only in 1910 by Matthew Hunter of New York. Titanium has excellent properties, including its non-corrosive nature and the ability to osseointegrate. The latter property was accidentally observed in 1952 by Per-Ingvar Brånemark, a Swedish physician studying blood flow and bone healing in rabbits. The titanium chambers placed into the shin bones of the rabbits fused. It led to “osseointegration”, as Brånemark coined it (35). Titanium proved the biocompatible material that eluded so many earlier attempts. With the improving success of titanium endosteal implants, subperiosteal implants fell out of favor.
Today, root-shaped endosteal titanium implants are the acceptable norm. The improvements in the material’s biocompatibility, osseointegration, and bone augmentation when insufficient supporting structures exist made implants ubiquitous.
History of the treatment for cleft lip and palate
The cleft palate and lip hold a unique place in the history of oral surgery. The developmental defect was known from the dawn of civilization and had a rich history of treatments with obturators, especially from the 16th century onward. Recent evidence indicates that both pharaoh Akhenaten (ruled between 1351-1334 BCE) and his famous son, King Tutankhamun (ruled 1334-1324 BCE), had a cleft palate (36). It is speculated that the famous Greek orator Demosthenes (384-322 BCE), had a left-side cleft palate and lip. He was said to have placed pebbles into his mouth. He practiced his speech on a beach to improve his oratory and overcome an impediment presumed to be stuttering or rhotacism, a mispronouncement of the sounds r and l. Another hypothesis holds that his speech impediment was due to a left-side cleft lip and palate and that the practice sessions on the beach were a way to try flat pebbles as ad hoc obturators (37). The observation on two busts of Demosthenes at the British Library that his upper left lip carries a hairline suture and underdeveloped lip muscle makes this argument more plausible.
The earliest description of cleft lip surgery comes from 390 CE in China. The patient, Weig Yang-Chi, had his cleft lip surgically corrected by the surgeon in the governor’s service of Hunan province. The defect was cut and sutured together, and the patient was kept for 100 days in bed on a diet of thin porridge without smiling or talking (38).
French surgeon Franco Pierre first described cleft lip and palate in 1556 (39). Franco was a contemporary of Paré, a fellow Huguenot who moved to Lausanne, Switzerland, to escape persecution. Published in Lyon in 1556, Franco describes the surgical treatment of the cleft lip, suturing and covering the wounds with a mixture of resin powders, Frankincense, Dragon’s Blood, mastic, and egg yolk (39).
Following the spread of syphilis in Europe after Columbus’ return and the French-Italian Wars, palatal perforation became common due to stage III syphilitic gumma. Therefore, a renewed interest in treating cleft palate appeared. The solution, for centuries, was non-surgical, using an obturator. The first description of an obturator comes from Amatus Lusitanus (1511-1568) in his 1560 edition of Curationium Medicinalium. The obturator was a “golden-headed nail” custom-made with a goldsmith for a luetic palate perforation (40). Just about the same time, in 1561, Ambroise Paré published his work on treating wounds and fractures in which he illustrated for the first time an obturator for the palate and instruments to place them (41). He calls it “ instrument pour la palais troué,” an instrument for the cleft palate. He has a sponge hanging from the nasal side to anchor it. Later models had a button-like structure that could be turned 90 degrees to hold the obturator in place. The term obturator appears only from 1575 (“obturateur du palais”) (42).
According to Karl Sudhoff (43), Franz Renner, a barber-surgeon from Nurnberg, described an obturator in 1557 made of multiple layers of leather (44). Over the next 150 years, the design of the obturator stayed the same. Pierre Fauchard had at least five designs, some to cover the palatal bone deficiency, and others were attached to upper dentures (45). Fauchard’s advantage over Franco or Paré was his extensive knowledge of dentistry.
The next significant advance in obturator design came from Christoph-Francois Delabarre (1784-1862), who created a better-fitting, mechanically adjustable obturator with a better palatal seal (46). Delabarre’s obturator was further improved in 1859 by Norman W. Kingsley (1829-1913), the founding dean of the New York College of Dentistry and the “Father of Orthodontics”. His obturator was covered with soft vulcanized rubber. Kingsley understood the function of the superior pharyngeal constrictor muscle during swallowing to create a natural seal around the obturator and hold the device in place. Many of Kingsley’s devices were award-winning, beautifully made works of art, a natural extension for a talented artist (47).
Parallel with obturators, with the advent of general anesthesia, surgical treatment of cleft lip and palate became the standard. It is beyond the scope of this section to cover the advances in surgical techniques to correct cleft lip and palate. The reader is invited to consult excellent reviews on this subject (48).
The history of oral surgery would only be complete with a retrospective view of the evolution of the specialty in general. It arose from two strands: general surgery treating pathologies of the head and neck and tooth extractions. Throughout its long history, a significant drawback in practicing any surgical intervention, extraction included, was a lack of anesthesia, sterility, and proper post-extraction care for swelling, bleeding, and infection. The solution to the above shortcomings came in short succession, starting with 1844-1846, nitrous oxide and ether anesthesia, respectively (Wells and Morton), gloves (1851, Maurice), the microbiological basis of infection (1864, Pasteur), aseptic surgery (1867, Lister), local anesthetic (1884, Koller), X-rays (1895, Roentgen), blood groups (1901, Landsteiner), and penicillin (1928, Fleming). Since 1919, oral surgery has become a specialty, the first and one of the most respected among dental specialties. With a combined medical degree, oral and maxillofacial surgeons today undertake one of the most delicate and essential interventions to improve form, function, and esthetics for patients.
- Breasted
- Shklar and Chernin (a) p.52
- Kiss
- Crossland
- Celsus p.443
- Geist-Jacobi
- Spencer p.251
- Becker
- Hoffmann-Axthelm p.44
- Abulcasis (a) p.172-5
- Idem p.176
- Abulcasis (b). p.186
- Hoffman Axthelm, p.129
- Chauliac p.71
- Paré (b). p.612-613
- ibid p.1199
- Ibid p.328
- Towers p.237
- Shklar and Chernin (b)
- Faggart and Garretson
- Bennion
- Fay
- Tomes
- Blackwell
- Breasted p.133
- Bhishagratna p. XVIII
- Sciappa p.395.
- Paré (b) p.210
- Tyler.
- Bobbio
- Pasqualini (a) (b)
- Maggiolo p.77, Pasqualini (b)
- Greenfield
- Linkow
- Albrectsson
- Hawass
- Bien
- Khoo
- Franco p.456-9
- Lusitanus p.42; Leibowitz
- Paré (a) p.261
- Pare (b). p.895
- Sudhoff
- Renner p.86-87.
- Fauchard p.305, p.320
- Delabarre, Vol II, Fig. 122
- Peck
- Hoffmann-Axthelm p.344
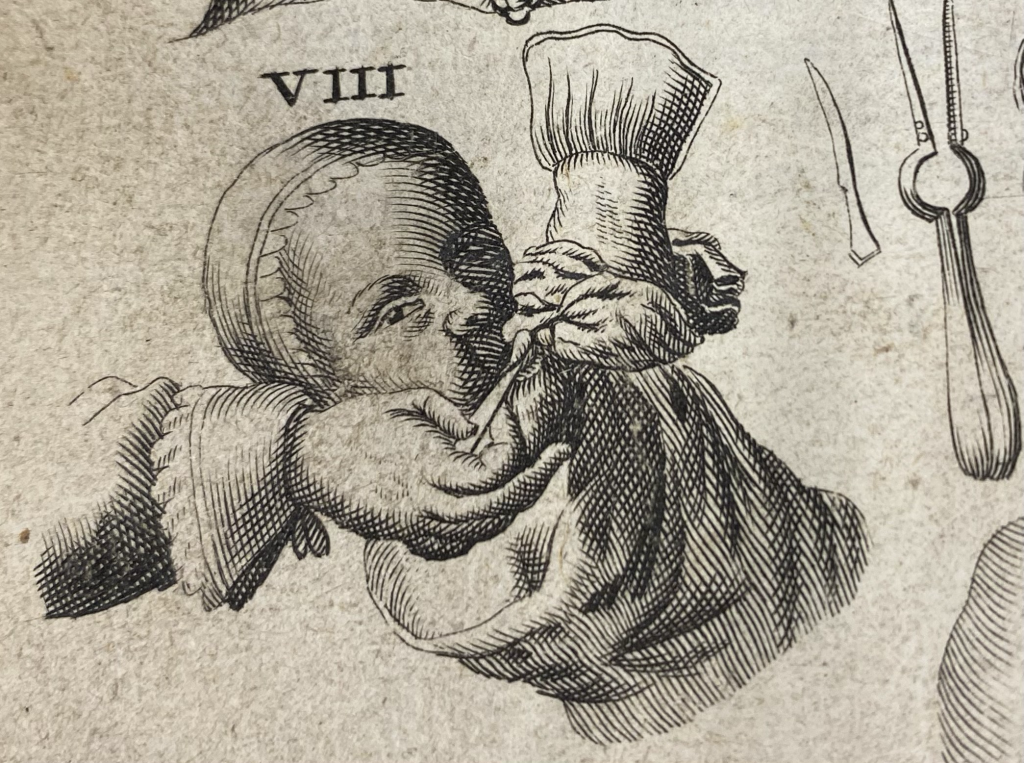
Tongue-tie or ankyloglossia are frequently seen in children with speech and nutritional impediments. The surgical solution is to free up the frenum (frenectomy, frenulectomy, frenotomy) to improve tongue movement.

Celsus drew attention to the dangers associated with surgical intervention in the sublingual area because of the closeness of the lingual veins (1). Celsus warns that “the tongue in some persons is tied down from birth to the part underlying it, and on this account, they cannot even speak. In such cases, the extremity of the tongue is to be seized with forceps, and the membrane under it incised, great care being taken lest the blood vessels close by are injured and bleeding causes harm”.
The lingual frenum is the most obvious site for intervention, but two lesser consequential freni are the upper and lower labial frenum. They connect the lip to the fixed gingiva at the midline between the central incisors. In some patients, the frenum helps create a space between the central incisors, called a diastema. Frenectomy followed by additional treatment can close the inesthetic gap.
The surgical procedure to loosen up the frenum involves a horizontal cut into the frenum, stretching the newly generated cut vertically, and suturing along the vertical edges (see images on the right).
Historically, frenectomy was performed either by midwives or surgeons. Since midwives were more frequently present, they undertook the surgery, often with complications, such as bleeding. Midwives were encouraged to perform in some parts of Europe (Passau), while in Heilbron, they were expressly prohibited. The danger of complications and severe bleeding from cutting into the lingual veins, ranula, or even death led Celsus, Galen, and Avicenna to urge caution.
Louis XIII was born with ankyloglossia. When his surgeon noticed that the dauphine had difficulty nursing, he promptly diagnosed and relieved it.
One of the great German surgeons, Iohannes Scultetus, provided detailed descriptions of the procedure (2) and the instruments involved (see image below).
Frenectomy is an ambulatory procedure, and today, it is routinely performed without any complications. For a detailed review of the history of frenectomy, see reference 3.
- Celsus, p.446
- Scultetus p.134
- Obladen
History of apicoectomy – root resection
When in a decayed tooth, bacteria penetrate through the root canal into the periapical space, causing infection, bone loss, abscess, and other pathologies; the solution for years was a root canal treatment and resection of the apical portion of the tooth. The procedure is called apicoectomy or apicectomy. The first clear description of the procedure appeared in 18811 by a French maxillofacial surgeon, Claude Martin (1843-1911). He states: Chronic alveolar-dental periostitis […] occurs at the top of the roots; it is enough to remove the small diseased portion to bring about complete healing. Drilling into the apical portion of the abscessed tooth to drain the pus, not necessarily to clean the necrotic tissue, was described a decade earlier.2
In 18803, John N. Farrar (1839-1913) of Brooklyn, NY, described the surgical intervention others performed: “A few operators […] pass through the alveolar process a bur drill of considerable size and cut away all the diseased territory, sac and bone“. Farrar, not a supporter of the “radical” procedure, came around by 1884. The same intervention was used a century earlier on teeth first extracted for root canal treatment; the diseased apex was resected, and the tooth was reimplanted. Phillip Pfaff (1713-1766), a German imperial dentist, and Thomas Berdmore (1740-1785), dentist to George III, King of England, used it with variable success.
The surgical method of root resection saw several improvements over the following decade. However, the goal stayed the same: removal of the infected apex and a good seal of the root canal to prevent reinfection from the oral cavity. A notable improvement came from the German surgeon Carl Partsch (1855-1932), active in the first third of the 20th century, whose surgical techniques varied whether the apical cyst was large (using marsupialization, Partsch 1 technique) or small (cystectomy, Partsch 2 technique).
One of the early options was apical tip resection with a low-speed rotary bur with water cooling or chipping the root tip with a chisel and mallet. Schamberg, in 1906, suggested a fissure, round, or rosehead bur to remove the apex, while Mead SV and Silverman SL in the 1930s were supporters of using a mallet and a chisel to avoid the overheating of the bone and the need for cooling.

Root canal therapy was performed before, during, or after apical resection surgery, and the type of endodontic material varied over the years from fast-setting cement with iodoform to laterally condensed gutta-percha and modern root-canal filling materials used today.
In the early 20th century, a retrograde amalgam filling was added to the resected tooth to provide a better seal.
Apicoectomies were frequent in the 1940s before fluoridation reduced dental decay and associated periapical complications. Today, the principle of sealing the periapical space from reinfection is still the same, but apicoectomies are far less frequent because of fewer cases and better restorative and endodontic materials. For a detailed history of endodontic surgery, see an excellent review by Gutmann and Gutmann.4
- Martin
- Smith
- Farrar
- Gutmann & Gutmann
When teeth become loose, avulsed, or overly taxed during mastication or need protection during contact sport, they need splinting to distribute the biting load on several adjacent teeth. The earliest evidence of splinting comes from 2500 B.C.E. from a mummy found at a Giza pyramid where two molars were connected with gold wire. Today’s interpretation of this find suggests a ceremonial role for the ligature to prepare the Pharaoh for the afterlife.
The Egyptians knew about splinting fractures. The Edwin Smith’s Papyrus (1550 B.C.) describes 48 trauma cases and methods to stabilize long bone fractures with braces or splints. It is unclear whether the Egyptians also used it to stabilize mandibular or maxillary fractures. The same surgical papyrus describes a “brace of wood padded linen” using the symbols shown in Figure 1. Case #7 in the papyrus is a patient with constriction of the mandibular ligaments. The patient is treated with a splint devised to keep the mouth open for feeding.
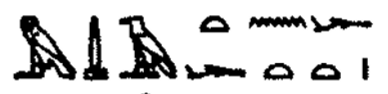
Figure 1. Hieroglyphs in the Edwin Smyth Papyrus for a linen-padded wooden brace used for splinting.1
A clear example of splinting periodontally loosened teeth comes from the 4th century B.C. Phoenicia (today Sidon, Lebanon). A 1901 excavation revealed a mandible with five anterior teeth with severe periodontal loss, splinted to each other with gold wire. The dexterity of the ligatures indicates considerable experience for the operator.2 (Figure 2).

Figure 2. Phoenician gold wire stabilization in 400 B.C. of five anterior teeth. (Image from Ref. 2).
Replacing missing teeth for ceremonial purposes using gold wire or bands to stabilize them was fashionable among high-cast young Etruscan females 2500 years ago.3
Islamic medicine has extensive surgical references. Abulcasis (936-1013), in the Encyclopedia of Medicine and Surgery, better known as Kitab al Tasrif, described gold wire splinting of teeth.4 That very same stabilization of loose teeth or even fractured jaws is also described in Ambroise Pare’s 16th-century masterpiece, Oeuvres. Paré was a barber-surgeon serving four French kings during major religious conflicts. His technique honed on the battlefield treated fractured jaws and loose or avulsed teeth. He suggested waxed threads or silver wires for loose teeth. Fractured maxillary and mandibular fragments were stabilized with interdental wire splinting, followed by a chin sling.

Figure 3. Silver wire stabilization of lower teeth in Abulcasis’ 11th-century book, Kitab al Tasrif. Image from a 1533 edition of the work.
Splinting of maxillary and mandibular fractures combined with extraoral stabilization was introduced in 1799 by Francoise Chopart (1743-1795) and Pierre-Joseph Desault (1738-1795) of France, and Rütenick, a Prussian regimental surgeon. The constant wearing of the harness caused chin lesions and soreness. By 1803, a French surgeon, Alexis Boyer (1757-1833), suggested intraoral fixation. A notable advance occurred in 1852 when Alphonse Robert (1801-1862) adopted a lead plate on the lingual surface of the lower teeth held in place by a silver wire passed through the floor of the mouth and tied extra orally over the chin.
In 1847, Gurdon Buck (1807-1877), a New York surgeon, proposed a wire suture passed through two holes next to the fractured bones. This procedure was improved with gutta-percha bite stabilization to keep the fractured fragments in occlusion. By the end of the Civil War, the interdental splint of hard rubber became a choice splinting system. In contrast, maxillary fractures still needed extraoral devices to ensure immobilization. 1822
Carl Ferdinand von Gräfe (1787-1840) created a steel forehead band (Figure 4.) with an intraoral device.
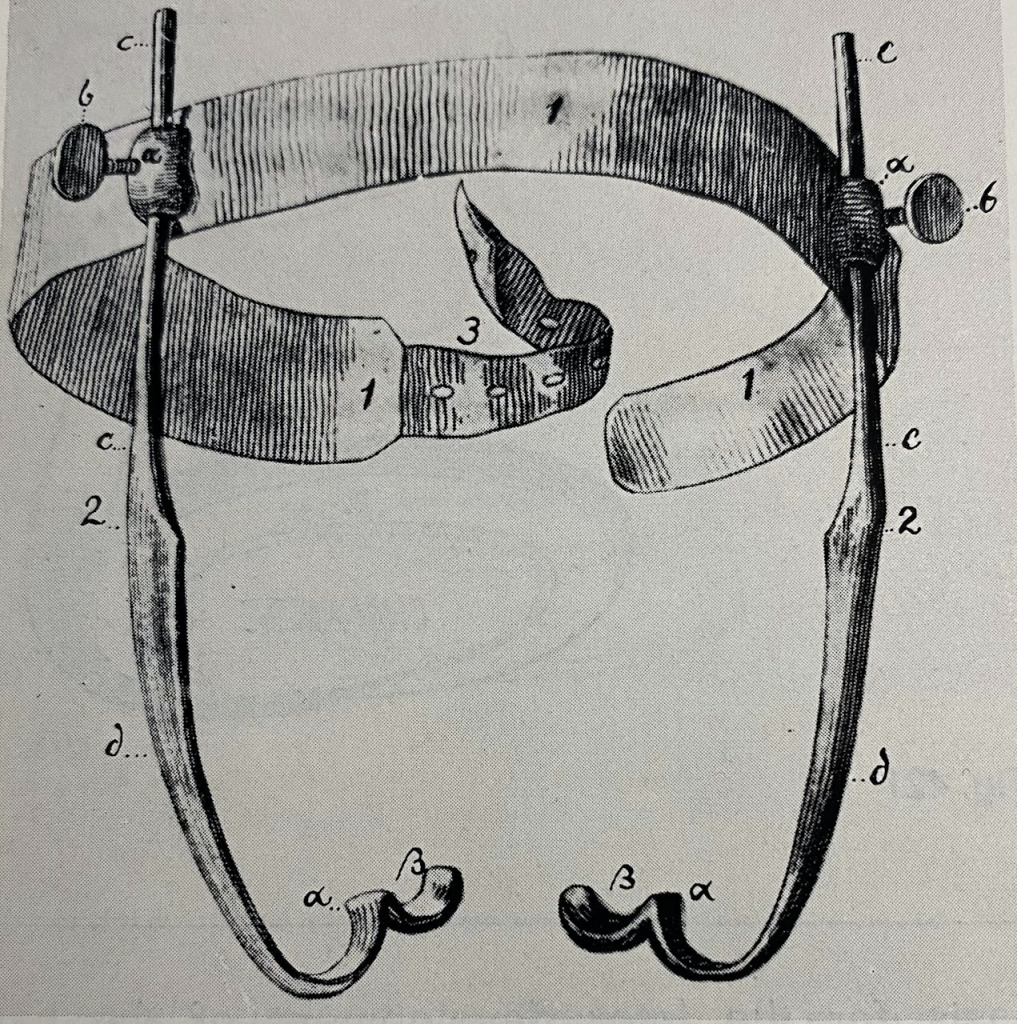
Figure 4. Steel forehead band designed by Carl Ferdinand von Gräfe.
Norman W. Kingsley (1829-1913), in 1880, attached a vulcanized rubber splint to the Gräfe device and simplified the extraoral system to a head cap.
The use of arch bars adapted to each jaw and held in place with wires tied around individual teeth was introduced in 1871 by Gurnell E. Hammond (1846-1926), a London dentist working with wounded at the Paris Commune. The Berlin dentist Carl Sauer (1835-1892) further improved this system using spring-action gold wire.
More recent interventions for splinting were expanded to include mouthguards to distribute bite forces for patients with bruxism and to protect teeth in contact sports. Mouthguards appeared first in the 1920s in professional boxing.5 By the 1960s, their use was mandated for Varsity and Intramural contact sports.
Dental brace splints for fixed orthodontics are covered in a separate section (see History of orthodontic braces). Today, splinting of teeth to stabilize traumatically avulsed and reimplanted teeth or those periodontally compromised use flexible or rigid bars held in place with composite resins. The materials used for splinting had gradually improved from linen-covered wood from Ancient Egypt to gold wire, gold band, silver wire, stainless steel wires, flexible nylon arch, and orthodontic brackets.
- Breasted
- Weinberger
- Becker
- Abulcasis
- Knapik et al.
Gloves were introduced after realizing that one needs to maintain a protective environment during surgery or childbirth to avoid infections and post-surgical complications. Although the literature incorrectly identifies William Stewart Halsted ordering the first pair of thin rubber gloves from Goodyear Rubber Company in 1889, this description is incorrect.
The first mention of a hand-protective device comes in 1758 from Johann Julius Walbaum, a German physician. (1)

Figure 1. (A) Walbaum (B) Description of the glove for delivery in Walbaum’s book. (C) Rendering of the glove. (Image courtesy of Historyofdentistryandmedicine.com.)
Walbaum describes: “The … device which I report upon here for the easing of delivery is a special glove which one draws over the hand with which one can turn and draw out the retained child. It is made of the blind gut (coecum) of sheep, which is 8 to inches long, and slit about 4 inches from the end. When I want to use it, I soften it in lukewarm water and draw it then over the middle finger, the ring finger, the little finger, and over the back of my hand, so that the index and the thumb remain uncovered. Next, I smear the glove and the bare parts of the hand with oil…”
A rendering of the glove is shown in Figure 1C. Walbaum was not concerned about sterility since the bacterial nature of the disease was unknown. His device is not entirely a glove in the usual sense since it covers only three fingers and the hand. He was concerned about having a good grip on an inverted fetus during delivery.
In 1808, Joseph Jacob Plenck, a Viennese dermatologist primarily concerned about the spread of syphilis to the operator, recommended that midwives applying mercury-containing ointment to a pregnant syphilitic patient should use a protective sheet (Aegrota ipsa vel alia femina sed manica munitas frictionem peragere potest. – The patient herself, or another woman, but with a protected sleeve, can apply [the mercury ointment]) He adds: Caveat obstetrix digitum vel manum vulnusculo vel ulcusculo læsam vaginæ venereæ , non nisi manica imbutam introducere – A midwife should beware of introducing an ungloved hand into the vagina of a venereally diseased patient if there are wounds or sores on her hands.

Plenck’s 1808 note to midwives to protect their hands when treating patients with syphilis
(see translation in the text above).
The glove Plenck refers to was not defined but could have been similar to Walbaum’s device made of sheep bladder, intestine, cloth, or leather. For a detailed description of the evolution of the surgical glove, the reader is directed to Renders-Pherson’s book (3).
In 1834, Richard F. Cooke, a physician, used oil of turpentine-solubilized caoutchouc to brush on his fingers to create an impermeable layer. In a letter to his mentor, a professor of surgery at Columbia University suggested that “a pair of India rubber gloves would be perfectly impenetrable to the most malignant virus” (4).
In 1838, the Charles Goodyear Rubber Company patented vulcanization. Ten years later, William Acton’s publication in 1848 in the Lancet demonstrated that caoutchouc can protect one’s hand (5). The next obvious step was the large-scale production of rubber gloves for surgeons performing dissections or working with patients suffering from venereal disease. Maurice Gabriel of France, working with the medical supply company of Varnout et Galante, was selling rubber gloves in 1851.
Thomas Foster of Streatham, England, secured a patent in 1878 to Manufacture Gloves for Surgical Operations. (6). He obtained a US patent the same year. However, surgeons were reluctant to adopt surgical gloves for fear of losing the fine tactile element during operations.

Figure. Thomas Foster – 1878 patent for rubber gloves.
The next step in the evolution of surgical gloves occurred more out of necessity rather than insight. William Halsted (1852-1922), a noted surgeon at Johns Hopkins University, requested in the winter of 1889 the Goodyear Rubber Company to prepare a thin rubber glove for his scrub nurse, Caroline Hampton, who developed a skin rash on her arm and hands due to handling chemicals like mercuric chloride. The gloves proved so successful that other surgical assistants handling instruments started to wear them during operations, and by 1893, surgeons also adopted them. Its spread was also due to Werner Zoege von Manteuffel, a German army surgeon, who published Gummihandschuhe in der chirurgischen Praxis (Rubber gloves in surgical practice) in 1897.
Several types of gloves were introduced at the end of the 19th century. In 1897, the surgeon Anton Wölfler of Prague used rubberized silk or leather gloves. The same year, Johannes von Mikulitz-Radeczki, a famous Polish-German surgeon, used steam-sterilized cotton gloves and, after sterilization, reused them. Whatever the material they were made of, surgical gloves became accepted in most surgical theaters at the beginning of the 20th century.
The use of examination gloves in dentistry was rare prior to the AIDS epidemic of the 1980s. In 1988, approximately 20% of US dentists used it, primarily to prevent transmission of the Hepatitis B Virus (HBV). In 1989, the Centers for Disease Control (CDC) guidelines included the need for personal protective equipment to prevent transmission of HIV/AIDS and Hepatitis B (7). Today, the CDC, the American Dental Association, and many state boards of dentistry have mandated the use of examination gloves in America. Such mandates are now standard worldwide.
Latex gloves were sterilized and reused. In 1964, the first disposable latex gloves were introduced. Talcum powder was added to make the donning of gloves easy. As both latex allergy and post-surgical talcum irritation of the wounds appeared, talcum-free and alternative materials were made available. Today’s gloves come in latex, neoprene, nitrile, synthetic or polyvinyl chloride.
- Walbaum
- Plenck
- Randers-Pherson
- Proskauer
- Acton p.589
- Forster
- CDC
References and notes on oral surgery
Acton W. On the advantages of solutions of caoutchouc and gutta percha in protecting the skin against the contagion of animal poisons. Lancet, Lond. II: 589, 1848. (Evidence that rubber can protect the hand from contagion).
Albrectsson, T, Brånemark PI, Hansson HA, Lindström J (1981). Osseointegrated Titanium Implants. Requirements for ensuring a Long-lasting, Direct Bone to-implant Anchorage in Man. Acta Orthop Scand. 52(2):155-70. doi: 10.3109/17453678108991776. (Osseointegration)
Abulcasis (a). (1532). Chirurgicorum Libri Tres. Strassbourg, p.172-176 – description of patient’s position, dental forceps and extraction instruments; p.177 – use of silver ligature to enhance loose teeth). This volume is combined with the work of Priscianus, Theodorus and Neuenra, Hermann von (1532). Rerum Medicarum Libri Quator. Argent Apud Ioannem Schottum. https://www.google.com/books/edition/Octauij_Horatiani_Rerum_medicarum_lib_qu/hF6rkGk6QLgC?hl=en&gbpv=1&dq=albucasis+Chirurgicorum+omnium&printsec=frontcover) (sedere infirmum inter manus tuas et caput eius in sinu tuo et rade molam et dentem. Translated: sit the patient between your hands and the patient’s head in your lap, and loosen up the gum around the tooth).
Abulcasis (b). (1778). De chirurgia. Tomus primus. Cura Johanneis Channing, natu et civitate Londonensis. Oxonii, 1778, p.186. (Illustration of extraction forceps for root tips.)
Becker, Marshall J. (2014). Dentistry in Ancient Rome: Direct evidence for extraction based on the teeth from excavations at the Temple of Castor and Pollux in the Roman Forum. Int. J. Anthropol. 29(4): 209-226. (https://thumbor.forbes.com/thumbor/960×0/https%3A%2F%2Fblogs-images.forbes.com%2Fkristinakillgrove%2Ffiles%2F2015%2F05%2FForumDentistsFig.1.jpg) (extractions in Roman Forum)
{kind=link}
Becker MJ, Turfa JM (2017). The Etruscans, and the History of Dentistry: The Golden Smile Through the Ages. Routledge monographs in classical studies. London; New York: Routledge, 2017. xxviii, 416. ISBN 9781138677913.
Bennion, Elizabeth (1986). Antique Dental Instruments. (General reference)
Bhishagratna, Kaviraj Kunja Lal, Editor, and translator. (1907). An English Translation of the Sushrata Samhita Based on Original Sanskrit Text. Vol I. Sutrasthanam, Introduction. Calcutta, p.XVIII.
Bien SM (1967). Why Demosthenes Mouthed Pebbles? Lancet, 2(7526):1152. doi: 10.1016/s0140-6736(67)90664. (Demosthenes used pebbles as an obturator for his cleft palate)
Backwell L, d’Errico F, Wadley L. Middle Stone Age bone tools from the Howiesons Poort layers, Sibudu Cave, South Africa,” Journal of Archaeological Science 35 (2008)1566–1580. doi:10.1016/j.jas.2007.11.006
Bobbio, Amadeo (1973). Maya, the first authentic alloplastic, endosseous dental implant. A refinement of a priority. Rev Assoc Paul Cir Dent. 27(1):27–36.
Breasted, James Henry (1922). The Edwin Smith Papyrus. The New York Historical Society Quarterly Bulletin VI (1), April 1922, 5-31. (description of the Edwin Smith papyrus).
Breasted, James Henry (1930). The Edwin Smith Surgical Papyrus. Volume 1. University of Chicago Press, Chicago p 230. (First mention of suture, hieroglyph “ydr” = means to sew, to stitch.). Case #10, p.230).
Breasted JH (1930). The Edwin Smith Surgical Papyrus, Vol. 1: Hieroglyphic Transliteration, Translation, and Commentary., Oriental Institute Publication, Chicago: The University of Chicago Press, 1930. ISBN 978-0-918986-73-3https://isac.uchicago.edu/research/publications/oip/edwin-smith-surgical-papyrus-volume-1-hieroglyphic-transliteration
CDC. Guidelines for prevention of transmission of human immunodeficiency virus and hepatitis B virus to health-care and public-safety workers. MMWR. 1989 Jun 23;38(6):1-37. (CDC guidelines for personal protective equipment in healthcare offices).
Celsus, Aulus Cornelius (1687). De Medicina, Lib VII, Cap XII, p.443. p. 446 (frenectomy), 1687) (Text on page 446: Lingua vero quibusdam cum subjecta parte a primo natali die juncta est; qui obid ne loqui quidem possunt. Horum extrema lingua vulsella apprehenda est, sub aeque membrana incidenda : magna cura habita, ne venae, que juxta sunt. Transl in 1938 by WG Spencer, part of Loeb Classical Library. : the tongue in some persons is tied down from birth to the part underlying it, and on this account they cannot even speak. In such cases, the extremity of the tongue is to be seized with a forceps, and the membrane under it incised, great care being taken lest the blood vessels close by are injured and bleeding causes harm.)
Chauliac, Guy de (1585). Chirurgia Magna Guido de Gauliaco (Laurentio Iouberto). Lugduni (Lyon). Interpretatio Dictionum Guidonis de Cauliaco cum Figuris Instrumentorum Chirurgicorum in eius opere memoratorum: mutuatis vtplurimum ex operibus Domini Paræi p.71
Crossland, Maurice (2004). The Officiers de Santé of the French Revolution: A Case Study in the Changing Language of Medicine. Med History. 48(2): 229–244. (1794 – Office de Sante, unification of physicians and surgeons in France).
Delabarra Christoph-Francois (1820). Traite de la partie mecanique de l’art du chirurgien-dentiste. Paris, 2 volumes. (New design of a mechanical obturator to better fit the soft palate, fig 1
Faggart, Harold L, Garretson, James E. (1945). Dr. James E Garretson and the First Hospital of Oral Surgery. Bull. Hist. Med. 17(4):360-367. (Garretson, established first specialty in 1869: oral surgery).
Farrar JN. Radical treatment of alveolar abscess. Dent Cosmos. 1880; 22:376-383. (Describes apicoectomy done by others. He is not yet supportive).
Fauchard, Pierre (1728). Le Chirurgien Dentiste, Vol II, p. 144-145. Paris. (Using forceps and detailed description, p 144-45; elevators p 143); vol 2. p. 292-338, plate 38, p.305; plate 39, p. 320.
Fay, Cyrus. (1825). No. XXII. Improved forceps for using dentists. Transactions of the Society, Instituted at London, for the Encouragement of Arts, Manufactures, and Commerce, 44; pp.167-181.
Forster, T. Improvements in the manufacture of gloves or coverings for the hands for use in surgical and other operations. British patent no. 1532, April 17, 1878. (First British patent for rubber gloves).
Franco, Pierre (1561). Traité des hernies contenant une ample declaration de toutes leurs especes. 2d Edition, Thibauld Payan. p. 456-459. (First to describe cleft lip and palate and surgical treatment of the cleft lip. His first edition appeared in 1556 and was entitled: Petit traite contenant une des parties principalles de chirurgie, laquelle les chirurgie-herniers exercent.)
Geist-Jacobi, GP (1896). Geschichte der Zahnheilkunde vom Jahre 3700 v. Chr bis zur Gegenwart. Verlag von Franz Pietzker, Tubingen. https://archive.org/details/geschichtederzah00geis/page/n6/mode/2up (opposite cover page – an ancient forceps).
Goldberg Hyman JV, Pinsky Theresa M, Jones Norine (1977). A short history of treating cleft lip and cleft palate. Bull Hist dent. 25(2):71-78. (general reference for cleft lip and palate surgery and palatala obturators.)
Greenfield EJ (1913). Implantation of artificial crown and bridge abutments. Dental Cosmos, 55(4):364-369. (Implant of a cylinder into the jaw and placement of a crown).
Gutmann JL, Gutmann MS. Historical perspectives on the evolution of surgical procedures in endodontics. J Hist Dent. 2010; 58(1):1-42. Good review of the history of endodontic surgery.
Halsted, William Stewart (1913). Ligature and Suture Material….also an account of the introduction of gloves…JAMA. 60(15):1119-1126. doi:10.1001/jama.1913.04340150001001 p.1123-1124. (History of the surgical gloves and sutures).
Hawass Zahi, Gad Yehia Z, Ismail Somia et al. (2010). Ancestry and Pathology in King Tutankhamun’s Family. JAMA, 303(7):638-647. (King Tut and his father had cleft palate).
Hoffmann-Axthelm, Walter (1981). History of Dentistry (Translated from German H.M. Koehler, Chicago:, Quintessence Publishing Co., Inc. p.44 (Using two fingers to extract teeth in Ancient China, Japan).; p.129 Guy de Chauliac is the first to describe the pelican); p.344 – History of Oral Surgery.
Khoo, Boo-Chai (1966). “An Ancient Chinese Text on a Cleft Lip.” Plastic and Reconstructive Surgery, 38:2, 89-91. (First description of surgical correction of cleft lip).
Kiss Laszlo (2015). Ecclesia abhorret a sanguine – Mikortol is? Orvosi Hetilap (Hungarian). 157(14): 554-557. DOI: https://doi.org/10.1556/650.2016.ho2541 ).
Knapik JJ, Marshall SW, Lee RB, et al. Mouthguards in Sport Activities History, Physical Properties and Injury Prevention Effectiveness. Sports Medicine, 2007; (2):117-144.
Leibowitz, Joshua O. (1958). Amatus Lusitanus and the Obturator in Cleft Palates. J. Hist Med. All. Sci. 13(4):492-503. (Lusitanus and the first obturator – good translation of Latin text and description of the first case).
Linkow, Lenard (1970). Theories and Techniques of Oral Implantology, MO, CV Mosby, St. Louis.
Lusitanus, Amatus (1560). Curationum Medicinalium, p.42-43. Venice. (First obturator described). (He calls the cleft palate: “ulcus palato innatum”.
Maggiolo M (1807). Le manuel de l’art du dentiste. (With an introduction of Jourdan M). p.77, Planche I, Item 11, 12,13,14).
Martin C. De la trépanation des extrémités radiculaires des dents appliquée au traitement de la périostite chronique alvéolo-dentaire. Association Française pour l’Avancement des Sciences. 10, Comptes-rendus de la 10e session, Alger, 1881. p.865-866. (First detailed description of apicoectomy).
Muffly, Tyler M, Tizzano Anthony P, Walters Mark D (2011). The History and Evolution of Sutures in Pelvic Surgery. J R Soc Med, 104:107–112. DOI 10.1258/jrsm.2010.100243 (History of sutures, in general).
Obladen, Michael. Much ado about nothing: Two Millenia of controversy on tongue-tie. Neonatology, 2010;97:83.89. (History of frenectomy).
Paré, Ambroise (1561) (a). La méthode curative des playes et fractures de la teste humaine, or “Treatment method for wounds and fractures of the human head.” p. 261-2. (One of the first description of an obturator, but without a name. He calls is: “instruments pour la palais troué” – instrument for the cleft palate.)
Paré, Ambroise (1628) (b). Les Oeuvres D’Ambroise Pare, Conseiller et premier chirurgien du Roi. Huictiesme Edition. Chapter XXVII. Les Instrumens propres pour arracher et rompre les dents. p.613 (surgical instruments).; p.1199A – mixture of egg yolk, oil of roses and turpentine – ”un digestif fait de jaune d’oeuf, huile rosat, et terebenthine; p.328 – hot cauterization replaced with ligature for bleeding. – Chez Nicolas Buon, Paris. (surgical instruments involved in extractions, pelican, forceps, elevators). (p.210 – sutures, threads, needles). p.895 – obturators. https://www.google.com/books/edition/Les_oeuvres_d_Ambroise_Par%C3%A9/wr8-AAAAcAAJ?hl=en&gbpv=1&dq=ambroise+pare,+oeuvres&printsec=frontcover.
Pasqualini U, Pasqualini ME Zampetti Paolo (2009) (b). The history of implantology. In: Treatise of implant dentistry: The Italian tribute to modern implantology. Ariesdue, Milan. (General reference for the history of implants and using clamshells for alloplasts). (Reproduction of Maggiolo’s implant – Fig. 30-34.
Pasqualini ME. (2000) (a). Un impianto alloplastico in una mandibola di 1300 anni. Ricerca istologica. Dent Cadmos. 11:57–62.
Peck, Sheldon (2012). Dentist, artist, pioneer. Orthodontic innovator Norman Kingsley and his Rembrandt portraits. JADA, 143(4):393-397.
Plenck, Johann Joseph. Doctrina de morbis sexus feminei. Viennae: Apud Joh. Georgium Binz, 1808. p.103-104. https://www.google.com/books/edition/Doctrina_de_morbis_sexus_feminei/rghfAAAAcAAJ?hl=en&gbpv=1&bsq=Caveat (first note to midwives to protect their hand against infection with syphilis)
Proskauer, Curt. Development and use of the rubber glove in surgery and gynecology. J. Hist Med All Sci, 1958; 13(3):373-381. Oxford University Press. Https://www.jstor.org/stable/24619258.
Randers-Pherson J. The Surgeons’ Gloves. Springfield, Illinois. Charles C. Thomas, 1960. (good review of the hisotry of surgical gloves).
Renner, Franz (1557). Ein Newwohlgegruendet nützliches und haylsames Handtbüch lein, etc. Nürnberg, Gabriel Heyn, p. 86-87.
Schiappa J, Hee R. Van (2012). From Ants to Staples : History and Ideas Concerning Suturing Techniques, Acta Chir Belg, 112, 395-402. (Using giant ants in ancient India as a substitute for sutures).
Scultetus, Johannes. Cheiroplothēkē: seu D. Joannis Sculteti… armamentarium chirurgicum XLIII. tabulis aeri elegantissimè incisis, nec ante hac visis, exornatum : opus posthumum… : cum triplici instrumentorum, curationum, rerumque memorabilium indice. Ex Officina Adriani Vlacq, Hagae Comitum, 1656. p 134, Tavola XXXVI, Fig. VIII. (instruments used for frenectemy).
Shklar, Gerald and Chernin, David (2001)(a). A sourcebook of dental medicine. p.52 – (Nei Ching, Chinese used extractions.)
Shklar G and Chernin D (2007)(b) Lorenz Heister and Oral Disease With the Original Text From His Papers
J Hist Dent, 55(2):68-74. (Lorenz Heister’s work, general reference);
Smith CS. Alveolar abscess. Amer J Dent Sci. 1871; 5(7):289-300. (description of apicoectomy by drilling into an abscess for drainage and removal of necrotic tissue).
Spencer, WG (1935). Celsus De Medicina (Vol 2). Book VI. 9. 5-10. I. Page 250-251. (This is a translation of Celsus’ work with alternating Latin/English pages). https://archive.org/details/in.ernet.dli.2015.185050/
The actual Latin and translated quote: “ Quod si dolor eximi eum cogit, et piperis semen cortice liberatum, et eodem modo baca hederae coniecta in [id] foramen dentem findit, isque per testas excidet. Et plani piscis, quam pastinacam nostri, tygona Gaeci vovant, aculeus torretur, deinde conteritur resinaque excipitur, quae denti circumdata hunc solvit.” Translated: But if pain compels its removal, a peppercorn without the tegument or an ivy berry without the tegument is inserted into the cavity of the tooth, which it splits, and the tooth falls out in bits. Also, the tail spine of the flat fish, which we call pastinaca, and the Greeks call trygon (sting ray), is roasted, pounded, and taken up in resin, and this, when applied around the tooth, loosens it. (the sting ray contains quick lime or calcium oxide in the tail bone, which has a similar structure to the tooth with a pulp and dentin-like substance).
Sudhoff, Karl (1926). Vom Alter des Gaumenobturators, Janus, 1924, 28, 451-54. Quotes: Renner, Franz, Ein Newwohlgegruendet nützliches und haylsames Handtbüch lein, etc. Nürnberg, Gabriel Heyn, 1557, pp. 86-87.
Tomes, John (1841). On the construction and application of forceps for extracting teeth. London Medical Gazette, Vol II:424-430. (design of anatomical forceps for extraction).
Towers, Joseph (1767). The Life of Bishop Aylmer: In. British Biography, Vol III, R Goadby, London, p. 237. (Bishop of London extracted one of his teeth to show Queen Elizabeth I that the extraction is not that painful).
Tyler M Muffly, Anthony P. Tizzano, and Mark D Walters The history and evolution of sutures in pelvic surgery. J R Soc Med. 2011 Mar 1; 104(3): 107–112. doi:10.1258/jrsm.2010.100243
Walbaum, Johann Julius. Wahrnehmungen von den Ursachen und Zufällen vieler schweren Geburten … Aus dem Französischen übersetzt, und mit neuen Handgriffen und Werkzeugen vermehret von D. Johann Julius Walbaum. Vol 1. 1758. Published as a supplement to the translation of Andre Levret’s 1747 original French work Observations sur les causes et les accidents de plusieurs accouchements laborieux, – Treatise on difficult deliveries. https://archive.org/details/b33014437_0001/page/462/mode/1up?q=Johann+Julius+Walbaum(First description of a protective glove)
Weinberger, BW. Further evidence that dentistry was practiced in ancient Egypt, Phoenicia, and Greece. Bull Hist Med 1946, 20:2, 188-195. https://www.jstor.org/stable/44441040.