by Andrew I Spielman
How to cite this page: Spielman, AI. History of Caries and Caries Prevention. In: Illustrated Encyclopedia of the History of Dentistry, 2023. https://historyofdentistryandmedicine.com/
Dental caries is the single most common chronic childhood disease (1). Just 70 years ago, it was the same in the developing world. But if we go back to the dawn of our civilization, we find a very different picture.
Throughout history, caries incidence varied with the availability and quality of food. In Western Europe during the Early Medieval period (V – XV-th century), caries rates ranged between 3% and 23% (2). A study of the famous Ice Man, also known as Ötzi, a 3,300 BCE individual found in the Alps between Austria and Italy, near Bolzano, shows a fully intact set of teeth, with severe occlusal attrition but only two cavities (7%)(3).

Ötzi, the Ice Man, reconstructed image, (from Wikimedia Commons).
Studies in England, for instance, looked at the incidence in different periods: Iron Age, Roman-British, Anglo-Saxon medieval, seventeen- and nineteen-century dentitions, and found a correlation between diet, availability, and sugar refinement (4,5,6,7). When sugar became abundantly available in the 16th century, excessive use led to blackening of the teeth (8), and by the early 19th century, caries incidence rates increased parallel with a change in the pattern for a more carbohydrate-rich diet (9). By the mid-19th century, the rates were almost similar to the 20th century.
The absence of dental caries does not mean our ancestors did not suffer from toothache. It was one of the most dreaded conditions.
As far back as 13,000 calendar years ago, we find the earliest signs of dental caries manipulation in Tuscany, Italy. Late Upper Paleolithic men managed to make the carious lesion shallower to be less retentive. (10).
Thirteen thousand calendar years ago, we find evidence of attempts to restore a cavity after the cavity was enlarged. The internal wall of dental cavities had bitumen, vegetable fibers, and probably hair adhering to it. (11). In graves from 9,000 calendar years ago, during the early Neolithic, in Pakistan, evidence of dental drilling using a bow drill and stone flints emerged. (12). Their attempt to make the carious lesion shallower and less retentive.
The British Museum holds 660 cuneiform Tablets with medical prescriptions dating back to the 7th century BCE. In 1920, Thompson R. Campbell published a translation of some of the texts indicating advanced knowledge of medicinal plants to suppress dental pain. “If a man’s teeth hurt, thou shalt take a musdimgurinna the white of its inside thou shalt enclose in wool, with oil [sprinkle (?), put it on his tooth]; male mandrake-root, *ammi -root, . . . storax, gum of galbanum, vinegar, . . . flour against his mouth (tooth) [thou shalt bind and he shall recover] (13,14, 15).
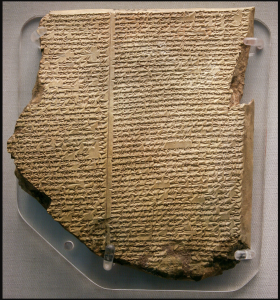
Cuneiform tablets like this are held at the British Museum dating back to the 7th century BC. Many contain description of medicinal plants used to treat dental pain. This particular one is the eleventh tablet of the Gilgamesh Epic of the Flood. (Image in the Wikimedia Commons).
Inscriptions on cuneiform tablets found by Henry Layard show that Assyro-Babylonians, as far back as 1800 BCE documented their suffering of toothache caused by the tooth worm. A highly poisonous plant root, Hyoscyamus nigra (henbane), was employed to fumigate the tooth to lessen the suffering(16). Even Ambroise Paré, the great surgeon of four French Kings, still believed in “tooth worm” and used acid or hot iron cauterization to remove the damaged area of the tooth in the hope of stopping the progress of caries. (17). Fauchard, the Father of Dentistry, suggested gargling with freshly collected urine (18) to reduce the rate of caries. The idea of a toothworm persisted well into the 18th century until Jacob Christian Schaffer disproved them (19). But, the dawn of a more rational approach to prevention and caries management appeared. Fauchard favored preserving the primary teeth as long as possible, and Robert Bunon in 1743, dedicated a whole book to oral hygiene and prevention (20).
The nature of the caries was still elusive at the beginning of the 19th century. In 1837 Joseph Linderer displayed the first histological section on a tooth, revealing how the softer dentin structure, once affected, can undermine the harder and still intact enamel (21). A breakthrough was accomplished in 1889 when an American, Willoughby Miller, completed his doctoral thesis on the chemo-parasitic nature of dental caries. Working under the guidance of Robert Koch in Berlin, Miller demonstrated that carbohydrate fermentation products of oral bacteria-produced acid, which dissolved the enamel (22). Miller’s ideas were not entirely original. In 1881, Underwood and Milles (23) proposed a similar theory and presented it at a World Congress in London. Miller made sure the ideas presented by Underwood and Miles were correct. The question of which specific oral bacteria were the main culprits had to wait until 1924 when J. Kilian Clark of St. Mary’s Hospital in London stumbled upon a strain of Streptococcus (24). While regular Streptococci were round, this strain mutated into a rod shape as the decay advanced, hence the name Streptococcus mutans. It took another thirty years before S. mutans was unequivocally identified as one of the main culprits. In 1954 Frank Orland of Notre Dame showed that when germ-free rats were given S. mutans and a cariogenic diet developed caries, while diet alone in germ-free animals did not. (25). This breakthrough led to predictions of developing a vaccine for caries. Those attempts, unfortunately, failed because caries pathogenesis proved more complex. We now realize also that acid production in the dental plaque is not a unique characteristic of Strep mutans. The “nonspecific plaque hypothesis” implies that the dissolution of the enamel results from the total net acid production in the biofilm (1). Other acid-producing bacteria, like S. sobrinus, Lactobacillus, and others, must be accounted for rather than a single pathogen. Only after fully understanding the oral microbiome will it provide the tools necessary to tame the most pervasive human bacterial infection.
A thoroughly mechanical solution to their treatment was well established when specific bacteria were identified. In 1908, Greene Vardiman Black, a preeminent restorative dentist at Northwestern University in Chicago, published cavity preparation guidelines, extension for prevention, and principles that dominated 20th-century clinical dentistry (26). So pervasive and unique to dentistry was this mechanical solution that, even 100 years later, antimicrobial solutions to caries were primarily adjuncts. Even though oral microbiology/immunology has emerged as the field to find a biological solution to caries through a vaccine or passive immunization, so far, attempts have failed. In the first two decades of the 21st century, we are also seeing the emergence of minimally invasive dentistry (2004) using agents that arrest caries and avoid unnecessary dental tissue loss while restoring it. Only when dentin, enamel, or whole tooth regeneration takes hold in dentistry, as it will in the next two decades, will dentistry finally treat carious lesions as an infectious disease and offer a biological solution to it, as all other branches of medicine do.
Greene Vardiman Black, The Father of Restorative Dentistry (1836-1912). Image in the Public Domain.
Breakthrough in science is often a chance observation. Although “chance favors only the prepared mind”, as Louis Pasteur stated, in 1843, Desirabode, Malagou Antoine, a French dentist, noticed that fluoride “fluate” hardens enamel against caries. He realized its potential for caries prevention. He suggested a homogenous paste made of “silicate or fluoride of lime and desiccated aluminum and inserted into the tooth and dried with a hot plunger” (27)
But the preventive effect of fluoride appears sporadically in a few papers most of the 19th century, especially as a tool for expectant mothers. Then in 1916, Frederick McKay observed mottled enamel in children in the Rocky Mountain region without understanding its cause. He publishes in Dental Cosmos an observational study with G. V. Black as the lead author (28). Suspecting the water supply, McKay sent water samples for analysis. They showed high fluoride levels. In 1929 Frederick McKay establishes a link between fluoride and caries resistance and mottled enamel (29). That was followed up by Trendley H. Dean publishing several seminal papers (30) on the relationship of fluoride, mottled enamel, and caries prevention, setting the stage for water fluoridation in many municipalities worldwide and significant reductions in the incidence of caries. Once H. Trendley Dean established the minimum level of water fluoridation, 1 part per million (ppm), to provide a protective effect against dental caries without dental fluorosis, water fluoridation of water was just a matter of time. In 1945 water fluoridation was introduced in Grand Rapids, Michigan, as a preventive measure against tooth decay.
Approximately 214 million Americans, about 75% of the US population, are exposed to water fluoridation today at a level that ranges between 0.7 and 1.5 mg per l. First marketed in 1895 by the Karl Frederick Toellner Company of Bremen, today, fluoride is available through drinking water, salt, toothpaste, milk, mouthwash, in the form of paste, gel, foam, rinse, solution, drops, tablets, and dentists’ applied topical fluoride via dental sealants and fluoride varnish. Over the years, every dollar invested in fluoridation saved $38 in dental treatment costs. Fluoridation is among the top five most impactful public health measures in the United States. As a result, loss of teeth leading to complete edentulism fell from 50% in 1960 to 13% in 2012.

Most toothpastes are fluoridate today.
Varnish, sealants, and silver diammine fluoride are different versions of the same aim: arrest initial decay, block bacterial access, and reduce retentiveness of pits and fissures. However, their history varies.
Previous attempts to seal the surface of teeth to prevent decay go back to the turn of the 20th century when Stebbins (31), Johann Frank (32), and W.D. Miller (33) suggested using silver nitrate as a protective agent on intact tooth surfaces. Even though silver has antibacterial effects, the procedure never took hold among practitioners, most likely due to the dark brown precipitation and unfavorable esthetic associated with it.
Soon after introducing the composite bonding agent, including Bis-GMA, Buonocore suggested its use as a sealant. The early generation of bonding agents did not adhere to the enamel sufficiently. Finally, in 1974 McLean and Wilson (34) introduced glass ionomer cement as a modern fissure sealant, with 84% remaining in place after one year and 78% after two years. Subsequent generations of sealants, and especially resin-based products, further improved the performance of these valuable preventive tools.
Fluoride varnish is a highly concentrated fluoride applied in a dental office. Such an application lasts a few days to weeks and needs reapplication. They were introduced in early 1980 in Canada, Western Europe, and Scandinavian countries. It contains a 1-5% fluoride salt (a silane) in a resin-based solution for fast drying. They are highly effective.
Silver diammine (not diamine) fluoride (SDF) is a clear liquid with a highly basic pH of 10.4 with strong antiquaries properties. It mixes the antibacterial properties of silver and the caries-arresting and remineralizing effect of fluoride (35). The role of silver as an anti-caries agent was known for over 100 years (36). In 1917 an ammoniacal silver nitrate solution was commercialized as Howe’s solution (37) to sterilize carious lesions. It was used for the next 50 years successfully.

SDF applied to a carious tooth in a child. The tooth does not need restoration, the SDF arrests the progression of the caries. Image from Dr. Theodore Croll. Reproduced with permission.
Today’s SDF was developed in Japan in 1969 at Osaka University partly in response to a chance observation that Ohaguro women in Japan had no cavities. The Ohaguro was a religious matrimonial custom among married Japanese women and some aristocrats in the Edo period before the Meiji restoration (1868-1912) (38). Ohaguro women painted their teeth black. Just as the shiny black lacquer box is considered beautiful, so did women with blackened teeth.

Ohaguro, a woodblock print by Kunisada I, c. 1823. Image in Public Domain.
Once abolished at the beginning of the 20th century, caries rates among Japanese women dramatically increased. Ohaguro teeth were achieved using a dye containing ferric acetate combined with vegetable tannins from gall nut powder and applied daily, creating a permanent black color to their teeth… and no cavities. The paint protected the teeth against bacterial access. SDF, which works similarly and hardens the enamel simultaneously, was approved in Japan in 1969 for caries prevention. In the US in 2014, the FDA approved it as a precipitating agent for dentin hypersensitivity only. Off-label, it is used as a caries arresting tool. A systematic review of 30-38% of SDF studies demonstrated an 81% caries arrest (39).

History of caries management in adults and children
Throughout the centuries, early and unscientific management of caries varied from the superstitious henbane fumigation of the tooth worm to extraction of the tooth under less than ideal conditions to the horrific hot iron cauterization to filling with lead, or if wealthy enough, with gold. Only in the 18th century and throughout the 19th century did restorative dentistry become dominant. With a few notable exceptions, like Hurlock’s 1742 work, A practical treatise on dentition, or the breeding of teeth in children, there was no focus on deciduous teeth (40).
In the late 19th century, traditional dentistry using amalgam and cavity preparation guidelines emerged. That approach to caries management lasted almost the entire 20th century. Parallel with invasive restoration techniques, several attempts were made for non-invasive approaches. Silver nitrate impregnation and silver diammine fluoride to arrest caries started as early as 1905. Fluoride and its preventive effect emerged at the beginning of the 20th century. By the early nineteen fifties, water fluoridation and, subsequently, fluoridation by other means started to take hold in the dental community, especially those dealing with children. As a result, pediatric dentistry emerged in 1940, and residency programs in that specialty appeared in the 1960s. Parallel with understanding the role fluoride had on an individual, an attempt to address large-scale oral preventive measures at a community level appeared and created a new field, Oral Public Health. Historically, the most significant task, water fluoridation, proved successful beyond the wildest expectations. Caries rates have significantly dropped worldwide due to it (41,42).
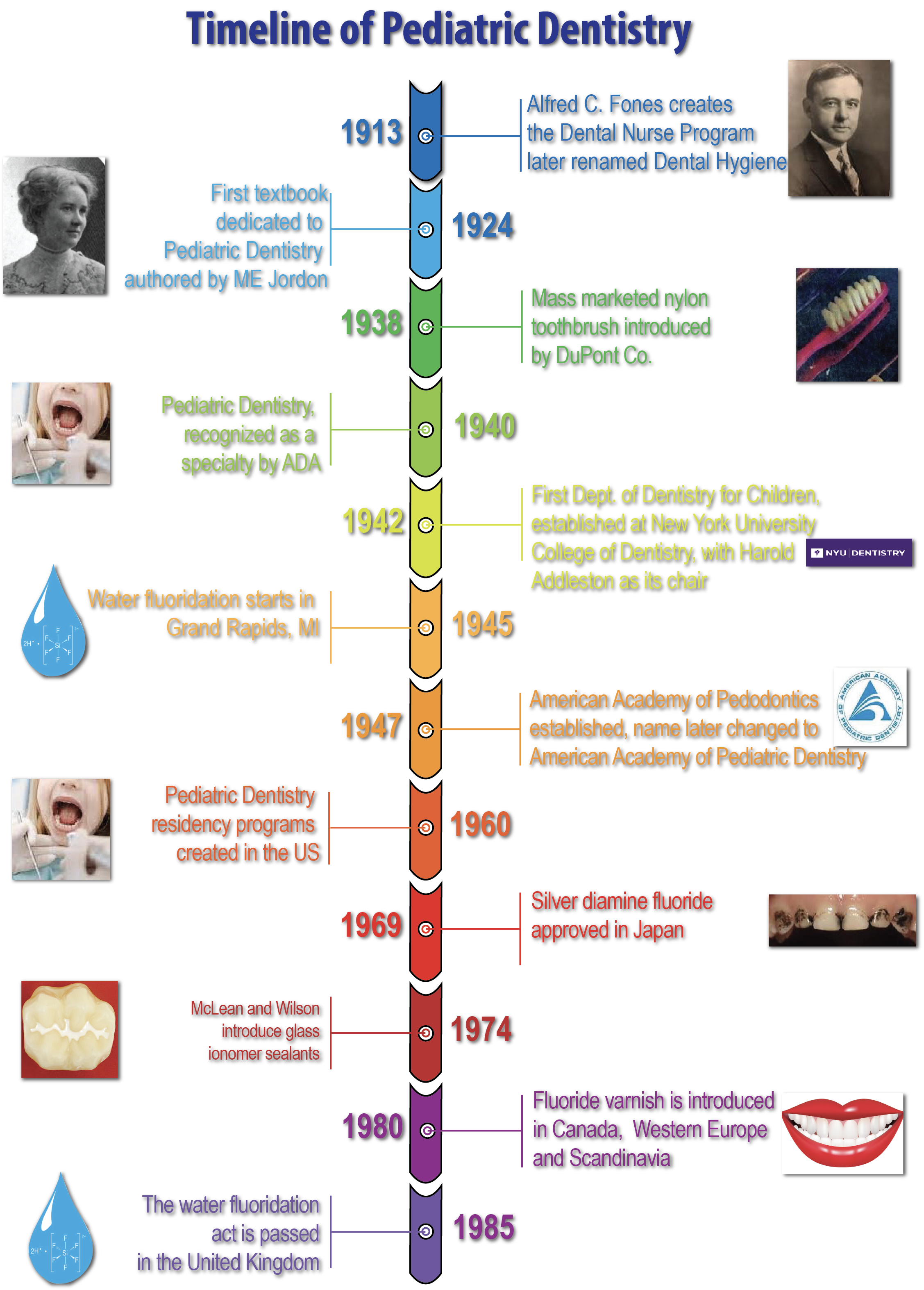
Timeline of Pediatric Dentistry – based, in part on the timeline at the American Academy of Pediatric Dentistry.
- 1. Pitts
- 2. Polet
- 3. Seiler 2013
- 4. More and Corbett 1971
- 5. ibid 1973
- 6. ibid 1975
- 7. Corbett and More
- 8. Hardwick,
- 9. More 1983
- 10. Oxilia 2015
- 11. Oxilia 2017
- 12. Coppa 2006
- 13. Thompson 1926
- 14. ibid 1923
- 15. ibid 1924
- 16. Sudhoff 1926
- 17. Paré p.395D, p.612
- 18. Fauchard Vol I. p.167
- 19. Schaffer
- 20. Bunon
- 21. Linderer p.189
- 22. Miller W.D. (b,c)
- 23. Underwood and Miles
- 24. Clark, J.K.
- 25. Orland, F.J.
- 26. G.V. Black105-210.
- 27. Desirabode, p.409.
- 28. Black and McKay
- 29. McKay
- 30. Dean
- 31. Stebbins
- 32. Frank, F
- 33. Miller W.D. (c) p.917
- 34. McLean and Wilson
- 35. Crystal and Niederman
- 36. Nishino
- 37. Howe
- 38. Ai
- 39. Gao
- 40. Hurlock
- 41. Petersen (a)
- 42. ibid (b)
References and notes on caries and caries prevention
Ai, S., Ishikawa, T., and Seino, A. (1965). “Ohaguro” traditional tooth staining custom in Japan. International Dental Journal 15, 426-441.
Black, Greene Vardiman (1908). A Work on Operative Dentistry. Chicago: Medico-Dental Publishing Company. Vol 2. p.105-210.
Black, Greene Vardiman and McKay, S. Frederick (1916) Mottled Teeth: An Endemic Developmental Imperfection of the Enamel of the Teeth Heretofore Unknown in the Literature of Dentistry. 58(2):129-156.
Bunon, Robert (1743). Essay sur les maladies des dents. Paris: Briasson Chaubert; De Hansy. p.237.
Bunting Russel W. (1928). The relationship of Bacillus acidophylus to dental caries. JADA 15, 1230-1233.
Clarke J. Killian (1924). On the bacterial factor in the etiology of dental caries. Brit J Exp Pathol 5:141–147
Coppa, A., Bondioli, L., Cucina, A. et al. Early Neolithic tradition of dentistry. Nature 440, 755–756 (2006). https://doi.org/10.1038/440755a
Corbett M. E. and Moore W. J. (1976) The distribution of dental caries in ancient British populations. IV. The 19th Century. Curies Res. 10, 401. ((caries rates in England V-XIX-c.)
Crystal, Y.O. and Niederman, R. (2019). Evidence-Based Dentistry Update on Silver Diamine Fluoride. Dent Clin North Am. 63(1):45-68.
Dean, Trendley H. (1938). Endemic fluorosis and its relation to dental caries. Pub. Health Reports 53:1443-52.
Desirabode, Malagou-Antoine (1843). Nouveaux elements complets de la science et de l’art du dentiste. 2 vol. po.409
Gao, S. S., Zhao, I. S., Hiraishi, N., et al. (2016). Clinical Trials of Silver Diamine Fluoride in Arresting Caries among Children: A Systematic Review. JDR Clinical & Translational Research, 1(3), 201–210. https://doi.org/10.1177/2380084416661474
Hardwick J. L. (1960) The incidence and distribution of caries throughout the ages in relation to the Englishman’s diet. Br. Dent. J. 108, 9-17. ( (caries rates in England V-XiXc.)
Hoffmann-Axthelm, Walter (1981). History of Dentistry, Quintessence Publishing 1981, Chicago, Berlin, Rio de Janeiro, Tokyo p. 319.
Howe PR. A method of sterilizing and at the same time impregnating with a metal affected dentinal tissue. Dental Cosmos 1917;59(9):891–904.
Hurlock, J. (1742). A practical treatise on dentition; or the breeding of teeth in children. C. Rivington, and S. Austen in St Paul’s Churc-yard and J. Hodges.
Fauchard, Pierre (1746). Le Chirurgien Dentist, 2d ed. Paris, Vol. i. p. 146.
Frank, Johann (1897). Argentum nitricum in der Zahnheilkunde. Oester.-Ungar Vierteljahrsschrift fur Zahnheilkunde, 13:364-370.
Linderer, C. J., Linderer, Joseph (1842). Handbuch der Zahnheilkunde. Berlin, Schlesinger’sche Buch und Musikhandlung. Vol I. p. 189, Tabl. XIII, Fig. 3.
McKay, Frederick S. (1929). The establishment of a definitive relation between enamel that is defective in its structure, as Mottled enamel, and its liability to decay. Dental Cosmos 71:747-755.
McLean, J.W., Wilson, A.D. (1974). Fissure sealing and filling with an adhesive glass-ionomer cement. Brit. Dent. J., 136:7, 269-276.
Miller, D. Willoughby (a) (1889). Die Microorganism der Mundhöhle. Die örtlichen und allgemeinen Erkrankungen welche durch dieselben hervorgerufen werden. Leipzig: Georg Thieme, p.364.
Miller, D. Willoughby (b) (1890). The micro-organisms of the human mouth: The local and general diseases which are caused by them. Philadelphia, The S.S.White Dental MFG. Co. p.364.
Miller, D. Willoughby (c) (1905). Preventive treatment of the teeth with special reference to silver nitrate. Dental Cosmos 47:64:913-922.
Moore W. J. and Corbett M. E. (1971) The distribution of dental caries in ancient British populations. I. Anglo-Saxon period. Caries Res. 5, 15 1. ( (caries rates in England V-XiXc.))
Moore W. J. and Corbett M. E. (1973) The distribution of dental caries in ancient British populations. II. Iron-Age, Romano-British and Mediaeval periods. Curies Res. 7, 139. ( (caries rates in England V-XiXc.))
Moore W. J. and Corbett M. E. (1975) The distribution of dental caries in ancient British populations. III. The 17th Century. Curies Res. 9, 163. (caries rates in England V-XiXc.)
Moore, W. J. (1983). Sugar and the antiquity of dental caries. In: The role of sugar in the aetiology of dental caries P. J. Holloway, PhD, BDS, (Editor). Journal of Dentistry, 11, No. 3, pp. 189-213. (caries incidence in England from iron age to 19th century).
Nishino M, Yoshida S, Sobue S, Kato J, Nishida M. Effect of topically applied ammoniacal silver fluoride on dental caries in children. Journal of Osaka University Dental School 1969;9:149‐55. (early use of silver diamine fluoride)
Orland, Frank J., Blayney, J. Roy, Harrison, R. Wendell, et al. (1954). Use of the Germ-free Animal Technic in the Study of Experimental Dental Caries: I. Basic Observations on Rats Reared Free of All Microorganisms. J. Dent. Res. 33(2), 147–174. https://doi.org/10.1177/00220345540330020201
Oxilia, G., Peresani, M., Romandini, M. et al. (2015). Earliest evidence of dental caries manipulation in the Late Upper Paleolithic. Sci Rep 5, 12150 (2015). https://doi.org/10.1038/srep12150
Oxilia G., Fiorillo F., Boschini F. et al. (2017). The dawn of dentistry in the late upper Paleolithic: An early case of pathological intervention at Riparo Fredian. Am. J. Phys. Anthropol., 163:446-461. doi: 10.1002/ajpa.23216.
Paré, Ambroise (1652). Oeuvres, XXV,. Lyon, 11th edition. (for prosthodontic treatment); tooth-worm (“les vers”), page 612, cauterization on page 395D).
Petersen PE, Lennon MA. (2004). Effective use of fluorides for the prevention of dental caries in the 21st century: the WHO approach. Community Dent Oral Epidemiol, 32(5):319–21.
Petersen PE, Ogawa H. (2016). Prevention of dental caries through the use of fluoride – the WHO approach. Community Dent Health, 33(2):66–8.
Pitts, N., Zero, D., Marsh, P. et al. Dental caries. Nat Rev Dis Primers 3, 17030 (2017). https://doi.org/10.1038/nrdp.2017.30
Polet, Caroline, Orban, Rosine, & Noël, R. (Ed.) (2001). Les dents et les ossements humains: que mangeait-on au Moyen Âge ? (Typologie des sources du Moyen Âge occidental; Vol. 84). Turnhout: Brepols Publishers. (Caries rates of 3-23% in Early Medieval Times).
Roger Seiler, Andrew I Spielman, Albert Zink, Frank Rühli. Oral pathologies of the Neolithic Iceman, c. 3,300 BC. European Journal of Oral Sciences, 2013; DOI: 10.1111/eos.12037
Schaffer, Jacob Christian (1757). Die eingebildeten Wurmer in Zahnen nebst dem vermeyntlichen Hülfsmittel wider dieselben – The imaginary Worms in Teeth and the alleged remedies against the same. Regensburg, p.42.
Sudhoff, Karl (1926). Geschichte Der Zahnheilkunde, 2d Ed. Leipzig. (henbane fumigation).
Stebbins EA. (1891). What value has argenti nitras as a therapeutic agent in dentistry?. International Dental Journal, 12:661‐70.
Thompson, RC. (1923). Assyrian medical texts. Humphrey Milford Oxford University Press; 1923. (From the Royal Library of Ashurbanipal, 7c. BCE)
Thompson, R.C. (1924). Assyrian Medical Texts: I. Proc R Soc Med. 1924;17)Sect Hist Med) 1-34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2201401/ (belongs to the Royal Library of Ashurbanipal, 7th c. BCE)
Thompson, R.C. (1926) Assyrian Medical Texts: II. Proc R Soc Med. 1926;19(Sect Hist Med):29-78. https://journals.sagepub.com/doi/pdf/10.1177/003591572601901703 (Royal Library of Ashurbanipal, 7th C. BCE)
Underwood AS and Miller WT (1881). Investigation into the effects of organisms upon teeth and alveolar portions of the jaws. Transactions of the International Medical Congress, vol 3. 523-529. London. (Demonstration of the chemo-parasitic theory of caries 17 years before Willoughby Miller).
Copyright 2022 ©HistoryofDentistryandMedicine.com